
Where to inject?
Which area you choose to inject into depends on various factors. The most important ones are: The site you use needs to be healthy and in good condition. Enough fatty tissue is another aspect which should be considered. Finally, the accessibility of the area plays a role.
Preferred areas and their absorption rates
Generally, the abdomen, thighs and buttocks are the most common sites(15): They can be reached easily and the fat layer here is rather thick. You have to find out yourself which area you prefer.
Please keep the following in mind:
- The fattier the injection site, the less likely you are to hit the muscle.
- Especially if you inject yourself, it is central that you can reach the injection site easily.
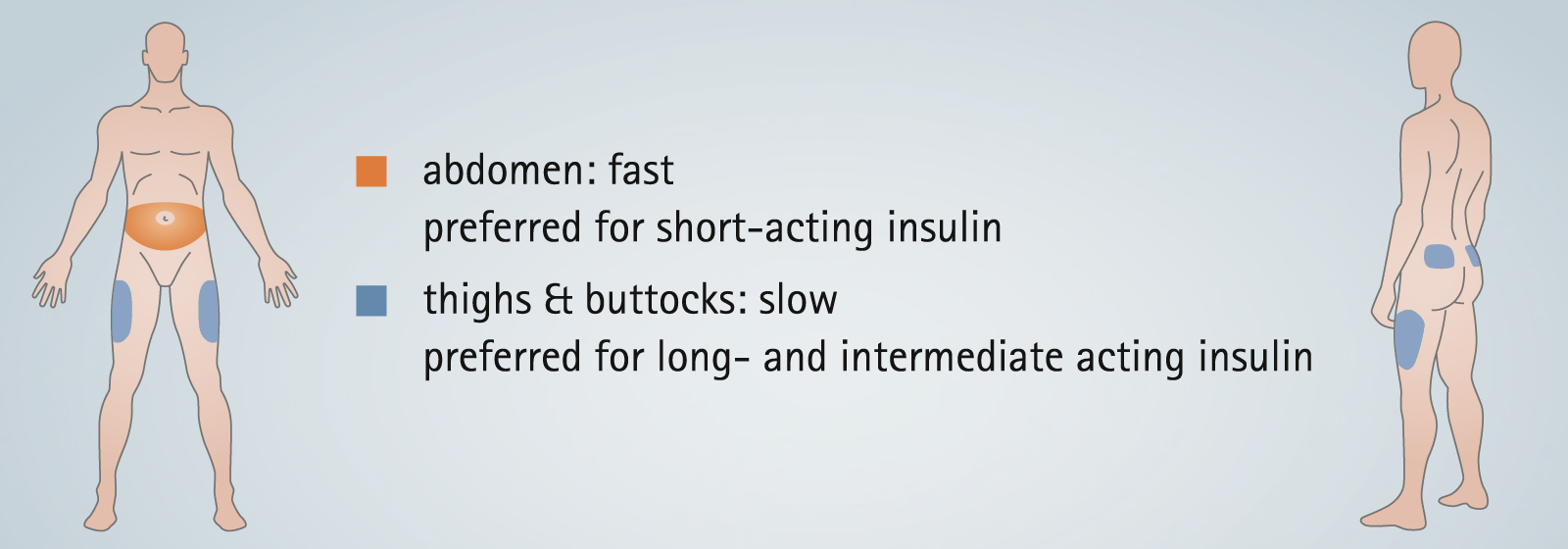
- The absorption rate has to be considered; insulin type and injection area should be compatible.
The pictures below show you the relation between different insulin types and the injection areas.(7, 8, 9)
Note: The upper arm is not recommended to use. This injection area is rather difficult to work with. Especially, since you would need a second person for the pinch up.
Furthermore, make sure that you avoid:
- lipos and scars
- moles and skin blemishes
- broken blood vessels.(3)
If you injected into the above-mentioned spots, the insulin would be absorbed irregularly.(3) Therefore, frequently checking for lipos is always sensible. If you detect any anomalies, please avoid them and contact your physician.
Tips: injection sites
✔ Always inject into normal, healthy skin.
✔ Keep an eye on the absorption rate.
✔ Find out which injection areas are the best for you
✔ Consider the insulin you are using as well as absorption rates.
Related topics
Sources
3. Frid A. et al., New Insulin Delivery Recommendations, Mayo Clinic Proceedings, September 2016; 90(9):1231-1255.
7. Bantle J. P. et al., Effects of the anatomical region used for injectable therapy injections on glycaemia in type 1 diabetes subjects. Diabetes Care 1993;16:1592-1597.
8. Frid A. et al., Clinically important differences in injectable therapy absorption from the abdomen in IDDM. Diabetes Research and Clinical Practice 1993;21:137-141.
9. Henriksen J. E. et al., Impact of injection sites for soluble injectable therapy on glycaemic control in type 1 (injectable therapy-dependent) diabetic people with diabetes treated with a multiple injectable therapy injection regimen, Diabetologia 1993;36:752-758.
15. Hirsch L. et al., Intramuscular Risk at insulin Injection Sites-Measurement of the Distance from Skin to Muscle and Rationale for Shorter-Length Needles for Subcutaneous Insulin Therapy, Diabetes Technology & Therapeutics, December 2014;16(12):867-873.